Anemia – Hemorrhage (Procedure-Associated Conditions): Introduction
:quality(80))
Anemia – Hemorrhage (Procedure-Associated Conditions): Introduction
Overview and Implications
Hemorrhage or hemorrhagic anemia refers to anemia secondary to acute blood loss associated with a medical or surgical procedure. Bleeding is a potential complication of any surgical procedure, and the risk is proportional to the size and complexity of the surgery. High blood loss is associated with certain types of surgery such as cardiac and liver surgeries, certain orthopaedic procedures (such as hip replacement) and obstetric surgery. Mortality may be greatly increased when severe bleeding occurs during the operative procedure (National Institute for Health and Care Excellence (NICE), 2014).
A search of patient safety reporting/alert systems uncovered the following incidents of hemorrhage for patients undergoing medical or surgical procedures:
- Hemorrhage after liver biopsy (National Patient Safety Agency (NPSA) & National Reporting and Learning Service (NRLS), 2009)
- Hemorrhage following removal of femoral catheter (NPSA & NRLS, 2010b)
- Hemorrhage from arteriovenous fistula (NPSA & NRLS, 2011)
- Hemorrhage following placement of gastrostomy (NPSA & NRLS, 2010a)
- Hemorrhage during dialysis (Veterans Affairs Central Office, National Center for Patient Safety, 2008)
- Hemorrhage during/following colonoscopy (Oregon Patient Safety Commission, 2015)
There is a relationship between pre-operative anemia and hemorrhage during surgical procedures. Iron deficiency is a common cause of pre-operative anemia and it should be corrected at prior to surgery to achieve optimal results (Gombotz, 2012; Theusinger et al., 2014; Theusinger et al., 2007). Bleeding that occurs in hospital as a result of a medical or surgical procedure is associated with increased morbidity, mortality and increased length of stay (Clevenger et al., 2015; Ferraris et al., 2012; Gombotz, 2012; Muñoz et al., 2016; Musallam et al., 2011; Spahn, 2010).
For additional information regarding Hospital Harm anemia – hemorrhage, please refer to theHospital Harm Improvement ResourceAnemia – Hemorrhage: Health Care / Medication Associated Condition.
Goal
Reduce the incidence of hemorrhage or hemorrhagic anemia secondary to medical or surgical procedures.
Table of Contents
- Anemia – Hemorrhage (Procedure-Associated Conditions): Discharge Abstract Database
- Anemia – Hemorrhage (Procedure-Associated Conditions): Importance to Patients and Families
- Anemia – Hemorrhage (Procedure-Associated Conditions): Clinical and System Reviews, Incident Analyses
- Anemia – Hemorrhage (Procedure-Associated Conditions): Measures
- Anemia – Hemorrhage (Procedure-Associated Conditions): Success Stories
- Anemia – Hemorrhage (Procedure-Associated Conditions): References
Current page: https://www.healthcareexcellence.ca/en/resources/hospital-harm-is-everyones-concern/hospital-harm-improvement-resource
 (img: https://a-ca.storyblok.com/f/850807391887861/084049412e/general-image-three.jpg)
(img: https://a-ca.storyblok.com/f/850807391887861/084049412e/general-image-three.jpg)
Hospital Harm Improvement Resource
Patients expect hospital care to be safe and for most people it is. However, a small proportion of patients experience some type of unintended harm as a result of the care they receive.
The Canadian Institute for Health Information (CIHI) and Healthcare Excellence Canada (HEC) have collaborated on a body of work to address gaps in measuring harm and to support patient safety improvement efforts in Canadian hospitals.
The Hospital Harm Improvement Resource (improvement resource) was developed by HEC to complement the Hospital Harm measure developed by CIHI. It links measurement and improvement by providing evidence-informed practices that will support patient safety improvement efforts.
The purpose of measuring quality and safety is to improve patient care and optimize patient outcomes. The Hospital Harm measure should be used in conjunction with other sources of information about patient safety, including patient safety reporting and learning systems, chart reviews or audits, Accreditation Canada survey results, patient concerns and clinical quality improvement process measures. Together, this information can inform and optimize improvement initiatives.
The improvement resource is a compilation of guidance linked to each of the clinical groups within the Hospital Harm measure to help drive changes that will make care safer. Through research and consultation with clinicians, experts, and leaders in quality improvement (QI) and patient safety, the improvement resource is intended to make information on improving patient safety easily available, so teams spend less time researching and more time optimizing patient care.
Using the improvement resource
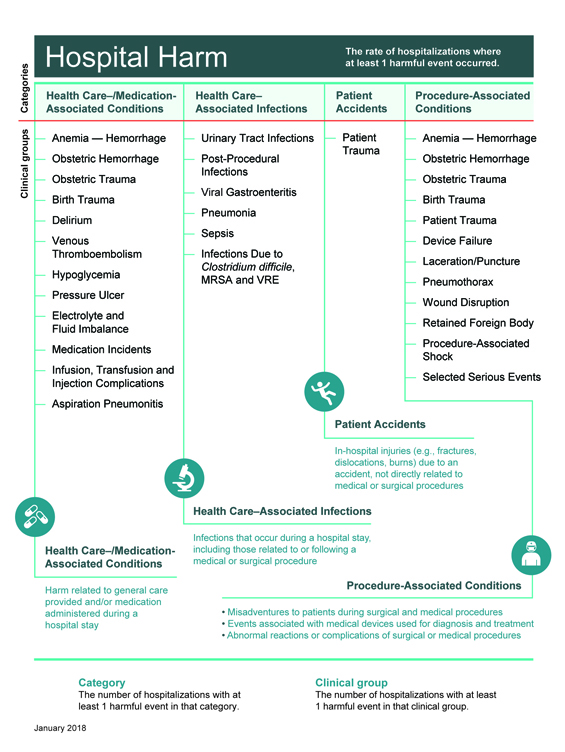
The layout of the improvement resource reflects the framework of the Hospital Harm measure (Figure 1) and focuses on actions that can be taken to decrease the likelihood of harm. The measure includes four major categories of harm; within each category is a series of individual clinical groups, or types of harm, each of which connects to evidence-informed practices for improvement.
For each clinical group, the improvement resource provides the following:
- an overview of the clinical group and goal for improvement
- implications for patients experiencing the type of harm and their importance to patients and family
- guidance for clinical and system reviews and incident analyses, including a list of resources specific to the clinical group
- guidance on measuring improvement
- success stories from organizations
- references.
Figure 1: Hospital Harm Measure Framework
 (img: https://a-ca.storyblok.com/f/850807391887861/1625902acd/hh-framework.jpg)
(img: https://a-ca.storyblok.com/f/850807391887861/1625902acd/hh-framework.jpg)
Definitions
As patient safety evolves it is important to be clear on the meaning and differences of specific words. For the purposes of the Hospital Harm measure, the following definitions apply:
- Harm:An unintended outcome of care that may be prevented with evidence-informed practices and is identified and treated in the same hospital stay.
- Occurrence of harm:Harmful event is synonymous with occurrence of harm.
- Hospital Harm Measure:Acute care hospitalizations with at least one unintended occurrence of harm that could be potentially prevented by implementing known evidence-informed practices.
For harm to be included in the measure, it must meet the following three criteria.
- It is identified as having occurred after admission and within the same hospital stay.
- It requires treatment or prolongs the patient's hospital stay.
- It is one of the conditions from the 31 clinical groups in the Hospital Harm Framework.
If you have any feedback or suggestions for the Improvement Resource, please send your ideas toinfo@hec-esc.ca
Table of Contents
- How to Use the Hospital Harm Measure for Improvement
- General Patient Safety Quality Improvement and Measurement Resources
- Learning from Harm
Resources
Anemia – Hemorrhage (Health Care / Medication Associated Condition): Discharge Abstract Database
Discharge Abstract Database (DAD) Codes included in this clinical category:
A01: Anemia – Hemorrhage (Health Care/Medication Associated Condition)
Concept | Hemorrhagic anemia or hemorrhagic disorders that require(s) blood transfusion, identified during a hospital stay, related to the health care delivered or therapeutic use of anticoagulants |
Notes |
|
Selection criteria | |
D62 | Identified as diagnosis type (2) AND Y44.2 in the same diagnosis cluster |
Exclusions | Y60–Y84 in the same diagnosis cluster |
Codes | Code descriptions |
D62 | Acute posthemorrhagic anemia |
D68.3 | Hemorrhagic disorder due to circulating anticoagulants |
Additional Codes | Inclusions |
Y44.2 | Drugs, medicaments and biological substances causing adverse effects in therapeutic use, anticoagulants |
Additional Codes | Exclusions |
Y60-Y84 | Complications of medical surgical care (refer toAppendix Aof theHospital Harm Indicator General Methodology Notes) |
Anemia – Hemorrhage (Procedure-Associated Conditions): Importance to Patients and Families
Even mild anemia leads to impaired functional capacity, physical performance and a reduced quality of life. As anemia worsens, tissue hypoxia and organ dysfunction become apparent (Clevenger et al., 2015). Hemorrhage is understandably alarming to patients and families. Not only may it be life-threatening, it complicates care and prolongs hospitalization.
Patients who experience hemorrhage may require blood transfusions (Spahn, 2010). Risks of blood transfusions include transmission of bacterial or viral infections, febrile transfusion reactions and transfusion-related acute lung injury (Mazer, 2014; Spahn, 2010; Theusinger et al., 2014).
Patient Stories
We are looking for a patient story related to hemorrhage or hemorrhagic anemia associated with a medical or surgical care. If you have one, please share it with the Canadian Patient Safety Institute atinfo@hec-esc.ca.
Anemia – Hemorrhage (Procedure-Associated Conditions): Clinical and System Reviews, Incident Analyses
Given the broad range of potential causes of anemia - hemorrhage,clinical and system reviews should be conducted to identify potential causes and determine appropriate recommendations.
Occurrences of harm are often complex with many contributing factors. Organizations need to:
- Measure and monitor the types and frequency of these occurrences.
- Use appropriate analytical methods to understand the contributing factors.
- Identify and implement solutions or interventions that are designed to prevent recurrence and reduce risk of harm.
- Have mechanisms in place to mitigate consequences of harm when it occurs.
To develop a more in-depth understanding of the care delivered to patients, chart audits, incident analyses and prospective analyses can be helpful in identifying quality improvement opportunities. Links to key resources forconducting chart auditsandanalysis methodsare included in theHospital Harm Improvement Resources Introduction.
If your review reveals that your cases of anemia - hemorrhage are linked to specific processes or procedures, you may find these resources helpful:
- American Society of Anesthesiologist.www.asahq.org
- American Society of Anesthesiologists: Practice Guidelines for Perioperative Blood Management (2015).https://anesthesiology.pubs.asahq.org/article.aspx?articleid=2088825
- British Committee for Standards in Haematology.https://www.guidelinecentral.com/summaries/organizations/british-committee-for-standards-in-haematology/
- Canadian Medical Association - CPG Infobase: Clinical Practice Guidelines.https://joulecma.ca/cpg/homepage
- Canadian Patient Safety Institute - Canadian Surgical Safety Checklist.https://era.library.ualberta.ca/items/c61d7d80-5197-4e1c-b89d-ce6054004d4d
- European Society of Anesthesiology.www.esahq.org
- European Society of Anaesthesiology: Management of severe perioperative bleeding (2017).https://journals.lww.com/ejanaesthesiology/fulltext/2017/06000/Management_of_severe_perioperative_bleeding__.3.aspx
- National Blood Authority- Australia.https://www.blood.gov.au/patient-blood-management-pbm#guidelines
- National Institute for Health and Care Excellence (NICE).www.nice.org.uk
- Network for the Advancement of Patient Blood Management - Haemostasis and Thrombosis.nataonline.com
- Ontario Regional Blood Coordinating Network- Bloody Easy for Healthcare Professionals.https://transfusionontario.org/en/documents/?cat=bloody_easy
- Thrombosis Canada.https://thrombosiscanada.ca/
- The British Society for Haematology.https://b-s-h.org.uk/guidelines/
- World Health Organization - Safe Surgery.https://www.who.int/patientsafety/safesurgery/en/
Anemia – Hemorrhage (Procedure-Associated Conditions): Measures
Vital to quality improvement is measurement, and this applies specifically to implementation of interventions. The chosen measures will help to determine whether an impact is being made (primary outcome), whether the intervention is actually being carried out (process measures), and whether any unintended consequences ensue (balancing measures).
In selecting your measures, consider the following:
- Whenever possible, use measures you are already collecting for other programs.
- Evaluate your choice of measures in terms of the usefulness of the final results and the resources required to obtain them; try to maximize the former while minimizing the latter.
- Try to include both process and outcome measures in your measurement scheme.
- You may use different measures or modify the measures described below to make them more appropriate and/or useful to your particular setting. However, be aware that modifying measures may limit the comparability of your results to others.
- Posting your measure results within your hospital is a great way to keep your teams motivated and aware of progress. Try to include measures that your team will find meaningful and exciting (IHI, 2012).
Anemia – Hemorrhage (Procedure-Associated Conditions): Success Stories
Best Practice in Patient Blood Management in a Surgical Patient Population
Sunnybrook Health Sciences Centre, Toronto, Ontario (Sunnybrook Health Sciences Centre, 2013)
The greatest predictor of whether a patient will need a transfusion is their preoperative hemoglobin level. The Holland Centre at Sunnybrook performs over 3,000 orthopaedic surgical procedures annually. In 2011, it introduced routine CBC (complete blood count) preoperative screening of all surgical candidates to identify anemic patients, manage potential anemia and refer high risk patients to the Blood Conservation Clinic for anemia optimization before surgery. All preoperative patients are given oral iron for one month. If patients are anemic, they are referred to the Blood Conservation Clinic (BCC) four to six weeks preoperatively for consideration of IV iron or Eprex. The project involved an interprofessional team that included Anesthesia, Hematology, Nursing, and Orthopaedic Surgeons. A preoperative blood conservation algorithm was designed and broad staff education was conducted. Patient education materials were also developed. Transfusion rates during the study period were 3.6% compared to 5.1% previously. The estimated cost-savings associated with fewer transfusions in this patient population was $75,000.
From blood transfusions, to heart surgery, to lung infections, Dr. Paul Hébert is doing research to improve the way we care for the sickest patients in the hospital
(Ottawa Hospital Research Institute, 2006)
Dr. Paul Hébert treats the sickest patients in The Ottawa Hospital – three of every 10 patients who arrive in the intensive care unit will never recover….While Dr. Hébert spends about half of his time trying to heal these patients one-by-one, the other half is spent on critical care research that is helping hundreds of thousands of patients in Ottawa and around the world….he found that patients treated aggressively with transfused blood had a higher death rate than patients whose doctors waited to order a transfusion.Read the full news article here.
Anemia – Hemorrhage (Procedure-Associated Conditions): References
Clevenger B, Mallett SV, Klein AA, Richards T. Patient blood management to reduce surgical risk.Br J Surg. 2015;102(11):1325-1337. doi:10.1002/bjs.9898
Ferraris VA, Davenport DL, Saha SP, Austin PC, Zwischenberger JB. Surgical Outcomes and Transfusion of Minimal Amounts of Blood in the Operating Room.Arch Surg. 2012;147(1):49-55. doi:10.1001/archsurg.2011.790
Gombotz H. Patient Blood Management: A Patient-Orientated Approach to Blood Replacement with the Goal of Reducing Anemia, Blood Loss and the Need for Blood Transfusion in Elective Surgery.Transfus Med Hemother. 2012;39(2):67-72. doi:10.1159/000337183
Institute for Healthcare Improvement (IHI).How-to Guide: Prevent Harm from High-Alert Medications. Cambridge, MA: IHI; 2012.http://www.ihi.org/resources/Pages/Tools/HowtoGuidePreventHarmfromHighAlertMedications.aspx.
Mazer CD. Blood conservation in cardiac surgery: Guidelines and controversies.Transfus Apher Sci. 2014;50(1):20-25. doi:10.1016/j.transci.2013.12.008
Muñoz M, Gómez-Ramírez S, Kozek-Langeneker S. Pre-operative haematological assessment in patients scheduled for major surgery.Anaesthesia. 2016;71(S1):19-28. doi:10.1111/anae.13304
Musallam KM, Tamim HM, Richards T, et al. Preoperative anaemia and postoperative outcomes in non-cardiac surgery: A retrospective cohort study.Lancet. 2011;378(9800):1396-1407. doi:10.1016/S0140-6736(11)61381-0
National Institute for Health and Care Excellence (NICE).NICE Publishes Draft Guidance on Tests for Bleeding Problems during and after Cardiac Surgery. London, UK: NICE; 2014.https://www.nice.org.uk/news/press-and-media/nice-publishes-draft-guidance-on-tests-for-bleeding-problems-during-and-after-cardiac-surgery.
National Patient Safety Agency (NPSA), National Reporting and Learning Service (NRLS).Haemorrhage after Liver Biopsy. London, UK: National Health Service; 2009. https://www.patientsafetyinstitute.ca/en/NewsAlerts/Alerts/Pages/AlertDetail.aspx?AlertID=NPSA013.
National Patient Safety Agency (NPSA), National Reporting and Learning Service (NRLS). Early Detection of Complications after Gastrostomy. London, UK: National Health Service; 2010a. https://www.patientsafetyinstitute.ca/en/NewsAlerts/Alerts/Pages/AlertDetail.aspx?AlertID=NPSA089.
National Patient Safety Agency (NPSA), National Reporting and Learning Service (NRLS).Haemorrhage Following Removal of Femoral Catheters. London, UK: National Health Service; 2010b. https://www.patientsafetyinstitute.ca/en/NewsAlerts/Alerts/Pages/AlertDetail.aspx?AlertID=NPSA014.
National Patient Safety Agency (NPSA), National Reporting and Learning Service (NRLS).Haemorrhages from Arteriovenous Fistula. London, UK: National Health Service; 2011.https://webarchive.nationalarchives.gov.uk/20120506001436/http://www.nrls.npsa.nhs.uk/resources/type/signals/?entryid45=94847&cord=ASC&p=1.
Oregon Patient Safety Commission.Patient Safety Alert: Colonoscopies and Red Dot Alerts for Anticoagulants. Portland, OR: Oregon Patient Safety Commission; 2015.https://oregonpatientsafety.org/news-information/news-information/action-alert-colonoscopies-and-red-dot-alerts-for-anticoagulants/553/.
Ottawa Hospital Research Institute (OHRI). From blood transfusions, to heart surgery, to lung infections, Dr. Paul Hébert is doing research to improve the way we care for the sickest patients in the hospital.OHRI Newsroom.http://www.ohri.ca/newsroom/story/view/751?l=en. Published June 1, 2006.
Spahn D. Anemia and Patient Blood Management in Hip and Knee Surgery: A Systematic Review of the Literature.Anesthesiology.2010;113(2):482-495. doi:10.1097/ALN.0b013e3181e08e97
Sunnybrook Health Sciences Centre.Leading Practices: Best Practice in Patient Blood Management in a Surgical Patient Population. Ottawa, ON: Health Standards Organization; 2013.https://healthstandards.org/leading-practice/best-practice-in-patient-blood-management-in-a-surgical-patient-population/.
Theusinger OM, Kind SL, Seifert B, Borgeat L, Gerber C, Spahn DR. Patient blood management in orthopaedic surgery: A four-year follow-up of transfusion requirements and blood loss from 2008 to 2011 at the Balgrist University Hospital in Zurich, Switzerland.Blood Transfus.2014;12(2):195-203. doi:10.2450/2014.0306-13
Theusinger OM MD, Leyvraz P-F MD, Schanz U MD, Seifert B PhD, Spahn DR MD,FRCA. Treatment of Iron Deficiency Anemia in Orthopedic Surgery with Intravenous Iron: Efficacy and Limits: A Prospective Study.Anesthesiology. 2007;107(6):923-927. doi:10.1097/01.anes.0000291441.10704.82
Veterans Affairs Central Office, National Center for Patient Safety.Bleeding Episodes DuringDialysis. Washington, DC: Veterans Affairs Central Office; 2008.https://www.patientsafety.va.gov/docs/alerts/BleedingEpisodesDuringDialysisAD09-02.pdf
Anemia – Hemorrhage (Procedure-Associated Conditions): Discharge Abstract Database
Discharge Abstract Database (DAD) Codes included in this clinical category:
D01: Anemia – Hemorrhage (Procedure-Associated Conditions)
Concept | Hemorrhage or hemorrhagic anemia associated with a medical or surgical procedure. |
Notes |
|
Selection criteria | |
D62 | Identified as diagnosis type (2) AND Y60-84 in the same diagnosis cluster AND documentation of blood transfusion (blood received indicator = 1) |
Codes | Code descriptions |
D62 | Acute posthemorrhagic anemia |
D81.0 | Hemorrhagic and haematoma complicating a procedure, not elsewhere classified |
Additional Codes | Inclusions |
Y60-Y84 | Complications of medical surgical care (refer toAppendix Aof theHospital Harm Indicator General Methodology Notes) |