Bringing Evidence to Life and Busting Myths through Stories
:quality(80))
Current page: https://www.healthcareexcellence.ca/en/resources/bringing-evidence-to-life-and-busting-myths-through-stories
Essential Care Partners are Essential for Patients [1] in All Health and Care Settings [2] : Bringing Evidence to Life and Busting Myths through Stories
We worked with essential care partners and patients to bring evidence to life and to bustedmyths through stories that show how essential care partners benefit care, experience, safety and outcomes, including during COVID-19.
An essential care partner is a person who provides physical, psychological emotional, and spiritual support, as deemed important by the patient. This care can include support in decision making, care coordination and continuity of care. Essential care partners can include family members, close friends or other caregivers and are identified by the patient or substitute decision maker.
Essential care partners are different to general visitors; they have a vital role in a patient’s care plan, including during the pandemic.
These stories were written by members and friends of the Essential Together Patient and Caregiver Advisory Group.
How Might We Bring Them Back Hôtel-Dieu Grace Hospital in Windsor has welcomed essential care partners since March 2020. Lisa is a Patient Advocate involved in setting up their Designated Care Partner program. Read Lisa’s story.
Find the Helpers Hôtel-Dieu Grace Hospital plans for their Designated Care Partner program to continue beyond the pandemic. Read this story from Janice Kaffer, CEO at HDGH.
Everyone Must Have Access Pamela is a mother and essential care partner to her son who has multiple complex disabilities and has fought to be allowed to be with her son as an essential care partner. Read Pamela’s story.
I am a Human Being Serena is a patient with a chronic condition that causes pain requiring emergency care. Read more about her experience visiting an emergency department alone.
Emi’s Story Emi is 6 years old, deafblind, requires full support for all daily living activities, and is frequently ill. His parents are his sole caregivers. See their story
[1] For the purposes of this report, “patient” includes clients and people living in long term care/nursing homes/advanced care homes, other congregate care facilities, and those receiving care in their home.
[2] Health and care settings refers to anywhere where people receive health and care. This can include hospitals, long-term care/nursing homes/assisted living and other congregate care settings as well as primary care, outpatient care and care in the home.
How Might We Bring Them Back
MYTH- Presence of Essential Care Partners increases infectious disease transmission.[1]
FACT- Essential Care Partners often learn to conduct medical procedures at home such as suctioning and administering medications. They also learn to carry out infection prevention and control procedures. Essential Care Partners are often eager to participate in safety training[2,3]as they are invested in the health and safety of their loved ones and for themselves. Essential Care Partners do not play a significant role in transmission.[4,5]They can safely be present if infection prevention and control protocols such as masking and screening are in place.[6-9]
Hôtel-Dieu Grace Hospital in Windsor has welcomed essential care partners since March 2020. More than750 people have gone through the orientation. Lisa is a Patient Advocate at HDGH and involved in setting up and running their Designated Care Partner program. Read Lisa’s story.
How Might We Bring Them Back
I wasn’t sure if I could even imagine it – no family presence or visitation. How would this work? How will families trust their loved ones would be okay? How will patients know they haven’t been abandoned?
How might we bring them back?
I placed myself in their shoes and all I could think about was the emotional distress this would create.
I began to frantically search for research, evidence and the “how to” for supporting essential care partners to come into hospital, despite the pandemic. This was important.
I found white papers that spoke about the emotional harm people had experienced after the first SARS pandemic. This couldn’t happen again.
I phoned a friend who is an epidemiologist, asking for any information that would support the importance of care partners supporting their loved ones in hospital during the pandemic.
At the same time, my phone was ringing off the hook; family members were missing their loved ones, they were concerned and they were feeling left out. They repeatedly expressed how unfair they believed the restrictions were. They were concerned about their loved one not understanding the separation and feeling abandoned; worried about their loved one being alone; concerned about their care needs being unmet as they (care partners) had been assisting with care. They were feeling anxious and it was difficult not being present – feeling in the dark. I empathized. I provided encouragement as much as possible, to comfort and put their minds at ease. Despite my efforts, I don’t believe their minds were ever at rest.
I had read the term, “essential care provider” and used it whenever I could. One day, I must have said it to the right person at the right time. “Essential care provider”, they said. “I like that”. The door was open and I stepped inside. I further explained the role and how critical it was for essential care providers to be supporting their loved ones.
A few days later, I was part of a team that was writing a guidance document for visitation during COVID-19. We were on our way.
Our family presence policy, written before COVID-19 used the term “Designated Care Partner.” This was chosen to reflect the patient’s choice as well as leaving the care and support provided, up to the patient and their care partner.
“How might we reintegrate designated care partners?” Asking staff and patients, both were equally afraid. How could we do this safely and without additional risk?
The answers included:
- Guidelines for health and safety, to ensure everyone was following all related site policies and public health measures
- Education and training for Designated Care Partners (DCPs)
- ID badge for DCPs
- Infection Prevention and Control (IPAC) education for DCPs
- Screening for safe entry and minimizing risk.
The DCP program was out of recognition that family and friends are integral to the patient’s care and healing. Family is defined by the patient and DCPs are trusted and valued members of the care team. DCPs are distinct from casual visitors because they know their loved one best and are uniquely familiar to subtle changes in their health or the way they feel.
The patient or substitute decision maker chooses the DCP. Once selected and the DCP commits to this role, they attend a 90 minute orientation. This session includes a review of the DCP roles and responsibilities, guidelines for safe entry and IPAC education. DCPs learn about the value of their partnership and their role as a member of the care team; they are informed that their responsibilities mirror some of the same responsibilities as staff, and understand the risk of exposure to COVID-19 and are asked to be mindful of this risk when at home or in community.
The IPAC portion includes information and interactive activities on proper hand hygiene, virus transmission, how to wear a mask and face shield, donning and doffing personal protective equipment.
Unit social workers meet the DCPs at the end of the session as a warm welcome to the unit.
The in-person orientation sessions offer DCPs a chance to ask questions and is foundational to establishing an on-going relationship.
DCPS are partners in the journey with their loved one and the vision is for the DCP program to continue beyond the pandemic.
- Guzzetta, Cathie. “Family presence during resuscitation and invasive procedures.” Critical Care Nurse 36, no. 1 (2016).
- Toronto Region COVID-19 Hospital Operations Table. “Access to Hospitals for Visitors (Essential Care Partners): Guidance for Toronto Region Hospitals (Acute, Rehab, CCC) During the COVID-19 Pandemic.’ October 2020. https://www.oha.com/Documents/Access%20to%20Hospitals%20for%20Visitors%20-%20 Oct%206.pdf .
- Alberta Health Service. “Community-based Service Resource Manual.” (2020), https://www. albertahealthservices.ca/assets/healthinfo/ipc/hi-ipc-community-based-services-resource-manual.pdf .
- Munshi et al. 2021. The case for relaxing no-visitor policies in hospitals during the ongoing COVID-19 pandemic. CMAJ. The case for relaxing no-visitor policies in hospitals during the ongoing COVID-19 pandemic | CMAJ
- Ontario Science Table. 2021. Impact of hospital visitor restrictions during the COVID-19 pandemic. Impact of Hospital Visitor Restrictions during the COVID-19 Pandemic - Ontario COVID-19 Science Advisory Table (covid19-sciencetable.ca)
- Wee et al. 2021. Containment of COVID-19 and reduction in healthcare-associated respiratory viral infections through a multi-tiered infection control strategy. Containment of COVID-19 and reduction in healthcare-associated respiratory viral infections through a multi-tiered infection control strategy - ScienceDirect
- Nguyen et al. 2021. IMPACT OF VISITATION AND COHORTING POLICIES TO SHIELD RESIDENTS FROM COVID-19 SPREAD IN CARE HOMES: AN AGENT-BASED MODEL: Controlling COVID-19 in care homes. IMPACT OF VISITATION AND COHORTING POLICIES TO SHIELD RESIDENTS FROM COVID-19 SPREAD IN CARE HOMES: AN AGENT-BASED MODEL: Controlling COVID-19 in care homes - ScienceDirect
- Wee et al. 2020. The impact of visitor restrictions on health care-associated respiratory viral infections during the COVID-19 pandemic: Experience of a tertiary hospital in Singapore. The impact of visitor restrictions on health care-associated respiratory viral infections during the COVID-19 pandemic: Experience of a tertiary hospital in Singapore - American Journal of Infection Control (ajicjournal.org)
- Passerelli et al. 2021. Asymptomatic COVID-19 in hospital visitors: The underestimated potential of viral shedding. Asymptomatic COVID-19 in hospital visitors: The underestimated potential of viral shedding - International Journal of Infectious Diseases (ijidonline.com)
Current page: https://www.healthcareexcellence.ca/en/resources/bringing-evidence-to-life-and-busting-myths-through-stories/find-the-helpers
Find the Helpers
MYTH- Presence of Essential Care Partners is nice to have, but doesn’t impact quality or safety
FACT- Having essential care partners present is a key part of patient and family centred care, which recognizes the mutually beneficial partnership between patients, families and healthcare providers. Patient- and family-centred care means recognizing the importance of family and caregiver presence and their participation in the care, quality and safety of patients.[1,2]
Hôtel-Dieu Grace Hospital in Windsor has welcomed essential care partners since March 2020. More than 750 people have gone through the orientation. HDGH plans for their Designated Care Partner program to continue beyond the pandemic as they continue to value and recognize the essential role of care partners. Read this story from Janice Kaffer, CEO at HDGH.
Find the Helpers
HDGH has been on a journey for a number of years to ensure that patient voice, family presence and a robust patient and family advisory culture (PFAC) is a foundation of our decision making, planning and service delivery. We have made great strides with a solid family presence policy crafted in partnership with our Patient and Family Advisory Council (PFAC), voting PFAC membership (2 members) on our Board of Directors which also has PFAC voice in our Board Quality of Care committee and numerous other improvements including family surveys and PFAC members as a resource to our inpatients and their families.
All of that is something I, as the CEO and also as a nurse for almost 40 years, have taken great pride in. It was my passion and my vision for what HDGH could be that gave rise to this evolution at our hospital and I am so pleased with the people, processes and the changes we’ve introduced to our organization and to our community. Don’t get me wrong, I have not done this alone – far from it – but leadership is about vision, about courage to do the right thing and the confidence to know that we’re headed in the right direction. Then the pandemic came and all of this was suddenly and without warning cancelled.
Cancelled family presence
Cancelled visitation
Cancelled caregivers who were with their loved ones every day ensuring their well-being on every level; physical, emotional, psychological and spiritual.
Cancelled.
I cannot tell anyone how hard that was to do. I, as the CEO who intentionally brought in patient families into our decision making, who envisioned our PFAC, is committed to family presence in our hospital, had to be the person to cancel it all. I was heartbroken and so were the leaders involved in dealing with the consequences of that decision. I stand by that decision as the right one at that time though because in the early days of the pandemic not one of us knew what we were dealing with nor did we understand the risks nor the mitigations that were possible. However, even though I knew it was the right decision, I knew I had to find a way as quickly as possible to change that decision for the betterment of our patients and their families. Ipad visits could only do so much – some of our patients truly needed their families to be with them for all the reasons listed above.
So I reached out to folks who know a lot more about what is possible than I did – I asked for help – I asked for advice – I asked for examples of where it was different and not surprisingly I got them all. I got help, advice and support from the caregiving community and as a result of that we made a different decision than CANCEL – we decided to INNOVATE – we decided to CREATE – we decided to TRY something new. As a result we introduced a new program into our hospital that, frankly, wouldn’t have come about without the pressure of this decision to not allow families in. We now have a Designated Care Partner program (DCP program) and it’s amazing!
Our patients have what they need from their families and our families are core to our high quality of care that we’ve been able to maintain through all the chaos of the pandemic. They are trained in the techniques needed to keep their loved ones safe and they understand their obligations and importance of staying true to the training. There have been a few bumps but those are to be expected and they are well worth it. We know so much now that it’s hard for me to imagine when we thought our only option was to CANCEL family presence in our hospital.
Our team will go over all the good stuff about the DCP program so I won’t do that but what I will say in closing is that I’ve taken away a few important lessons from this past year and one of them is this; When your heart and your soul tell you something isn’t right about what you’re doing – listen closely to that voice and find the helpers – they are always there and willing to help you find the way forward. I, along with our team, count ourselves among the helpers now and will happily help/support anyone who asks for it.
- Institute for Patient- and Family-Centered Care. “Patient-and Family-Centered Care.” (2010), https://www.ipfcc.org/about/pfcc.html .
- Frampton, Susan B., Sara Guastello, Libby Hoy, Mary Naylor, Sue Sheridan, and Michelle Johnston-Fleece. “Harnessing evidence and experience to change culture: a guiding framework for patient and family engaged care.” NAM Perspectives (2017).
Everyone Must Have Access
MYTH- Presence of Essential Care Partners is nice to have, but doesn’t impact quality of care
FACT- Impact of restrictive family presence policies has demonstrated risks to patient care, safety, and outcomes, including increased medical errors and inconsistencies in care, especially for those who are medically complex or vulnerable.[1,2]
Pamela is a mother and essential care partner to her son who has multiple complex disabilities. During the pandemic, Pamela has fought to be allowed to be with her son as an essential care partner. Read Pamela’s story.
Everyone Must Have Access
My son is 15, a sweet and joyful child who has multiple complex disabilities. Just before COVID-19 hit Canada, he experienced a seizure that caused an injury to his lip. His caring group home support staff took him to the hospital at our request, where we raced to meet them. Once we arrived, he had been seen by an Emergency Room physician, who advised the group home staff that “it would take too many resources to stitch his lip and we should just let it heal on its own,” despite the fact that it was painfully split open. Questioning the need for additional resources, I was told that because he wouldn’t stay still for the stitches they would have to sedate him, which would require staff from other areas of the hospital. As caring as the group home staff was, they accepted the doctor’s assessment at face value and were prepared for him to be discharged. As his mother and essential care partner, I challenged the advice and asked for a second opinion, knowing that all too often people with intellectual disabilities are treated differently from their neurotypical peers; in school, in access to services, and yes, in healthcare.
Our second opinion yielded what I already knew; OF COURSE he needed stitches, just as any other child who presented with the same injury would receive. The “additional resources” were gathered, and because we were present and advocated on his behalf in a situation where he was unable to advocate for himself, he received the stitches that his younger non-disabled brother would have received without question.
I wonder what the outcome would have been if this incident occurred in April 2020, when I was considered “non-essential” to my son.
There is an intersectionality in this story between essential care partners, congregate care staff and the healthcare system. Everyone in a congregate care setting, and everyone who enters an ER, must have access to their essential care partners to ensure they receive the treatment and care they require and rightfully deserve.
- National Collaborating Centre for Methods and Tools. “Rapid Review: What Risk Factors are Associated with COVID-19 Outbreaks and Morality in Long-term Care Facilities and What strategies Mitigate Risk?” (October 2020).
- Cacioppo, John T., and Louise C. Hawkley. “Social isolation and health, with an emphasis on underlying mechanisms.” Perspectives in biology and medicine 46, no. 3 (2003): S39-S52.
I am a Human Being
MYTH- Presence of Essential Care Partners is nice to have, but doesn’t impact quality or safety
FACT- Evidence continues to grow that demonstrates that the presence of essential care partners improves the safety, quality, and experience of care, including reducing readmissions to hospital,[1]and decreasing anxiety and stress for patients, essential care partners, and staff.[2-5]
Serena is a patient with a chronic condition that causes pain requiring emergency care. Read more about her experience visiting an emergency department alone.
I AM A HUMAN BEING
I am a Human being
I live with pain every single day of the year
Diagnosing me & my parents at the time of my birth devastated them
I would be spending the rest of my days in pain
Sick Kids Hospital became my second home as a child
and
Scarborough Grace Hospital became my second home as an adult that saved me...Why?
Because of a protocol
My pain is so real and the protocol helped advocate for me
IV, Oxygen and pain meds
IV, Oxygen and pain meds sounds simple but yet
So challenging to receive basic care
Oh wait, is it because I am not dressed up? Don’t I look approachable at 4am in the morning?
...sorry, let me brush my hair
I apologize for looking like I just rolled out of bed
...i don’t want to be here but the pain is too much
The stress, the anxiety...I’m here because I need help...please…
Will you help me? I’ve been here for hours
“It’s very unusual, you don’t look like you’re in pain”...that’s because I’m used to it
But not the intensity
...Please don’t think I'm a drug seeker, please don’t think I’m a drug seeker…
Do you have a protocol? Can you help? My list of meds is on there
It would be nice to see a change after 48 years or even after 111 years
Yes, that was my boyfriend who dropped me off
but the pain was too much for him to witness
So I am here alone
Fending for myself, hoping someone understands
What am I going to tell work again?
I hope they understand this time...I don’t want to be let go again
School is going to fail me because my paper was due
I don’t want to start the semester over again
Oh no! Rent is due next week and my finances are not enough
I can’t stay here, I must go back to work
Daycare will never understand so I will have to keep my daughter enrolled
Now I have to call my sister to help and she has work
I feel lonely...like I have no control
Maybe it’s best that I speak to a social worker
Empathy is all we ask from you
All conscience and unconscious biases are real but
I am a Human being
- S. Department of Health and Human Services. “New HHS Data Shows Major Strides Made in Patient Safety, Leading to Improved Care and Savings.”, 2014, https://innovation.cms.gov/files/reports/patient-safety- results.pdf .
- Belanger, Mary Anne, and Sandra Reed. “A rural community hospital’s experience with family-witnessed resuscitation.” Journal of emergency nursing: JEN: official publication of the Emergency Department Nurses Association 23, no. 3 (1997): 238.
- Helmer, Stephen D., R. Stephen Smith, Jonathan M. Dort, William M. Shapiro, and Brian S. Katan. “Family presence during trauma resuscitation: a survey of AAST and ENA members.” Journal of Trauma and Acute Care Surgery 48, no. 6 (2000): 1015-1024.
- McClenathan, CPT Bruce M., COL Kenneth G. Torrington, and Catherine FT Uyehara. “Family member presence during cardiopulmonary resuscitation: a survey of US and international critical care professionals.” Chest 122, no. 6 (2002): 2204-2211.
- Davidson, Judy E., Karen Powers, Kamyar M. Hedayat, Mark Tieszen, Alexander A. Kon, Eric Shepard, Vicki Spuhler et al. “Clinical practice guidelines for support of the family in the patient-centered intensive care unit: American College of Critical Care Medicine Task Force 2004–2005.” Critical care medicine 35, no. 2 (2007): 605-622.
Current page: https://www.healthcareexcellence.ca/en/resources/bringing-evidence-to-life-and-busting-myths-through-stories/emi-s-story
Emi’s Story
MYTH- Presence of Essential Care Partners is nice to have, but doesn’t impact quality or safety
FACT- Essential Care Partners are a constant part of a patient’s care journey and know them best. They play a significant role in providing and supporting care, and should be recognized.[1,2]Restrictive policies during the pandemic have led to increased caregiver distress and isolation.[3,4]
Emi is 6 years old, deafblind, can’t hold his head up, sit, stand or walk by himself and requires full support for all daily living activities. He suffers from a sleep disorder and is frequently ill. His parents are his sole caregivers. See their story
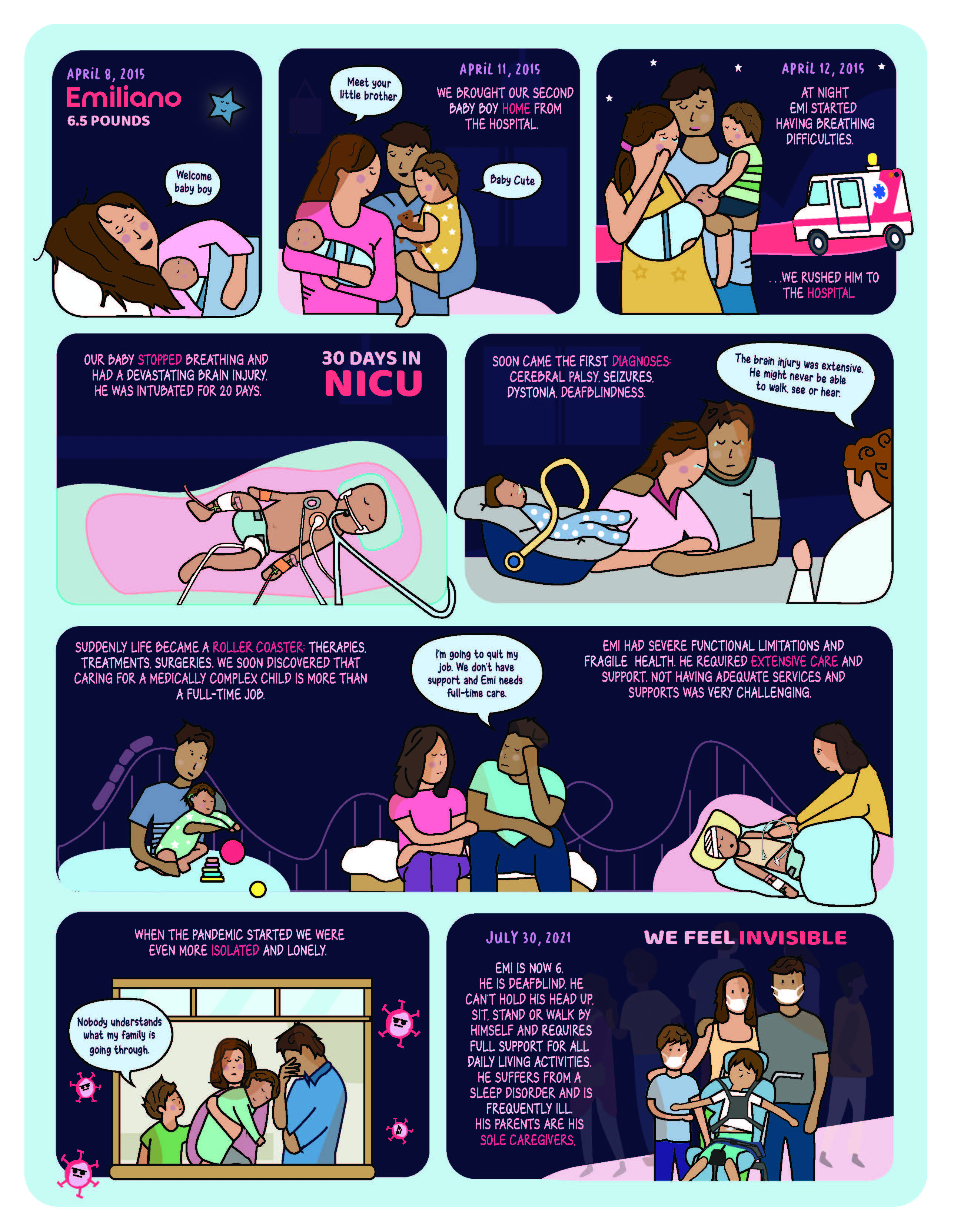
Transcript of Comic
April 8, 2015:Emiliano 6.5 pounds Welcome baby boy
April 11, 2015:We brought our second baby boy home from the hospital. Meet your little brother Baby Cute
April 12, 2015:At night Emi started having breathing difficulties. … We rushed him to the hospital
Our baby stopped breathing and had a devastating brain injury. He was intubated for 20 days. 30 days in NICU
Soon came the first diagnoses:Cerebral palsy, seizures, dystonia, deafblindness. The brain injury was extensive. He might never be able to walk, see or hear.
Suddenly life became a roller coaster:Therapies, treatments, surgeries. We soon discovered that caring for a medically complex child is more than a full-time job. I’m going to quit my job. We don’t have support and Emi needs full-time care. Emi had severe functional limitations and fragile health. He required extensive care and support. Not having adequate services and supports was very challenging.
When the pandemic started we were even more isolated and lonely. Nobody understands what my family is going through.
July 30, 2021:Emi is now 6. He is deafblind. He can't hold his head up, sit, stand or walk by himself and requires full support for all daily living activities. He suffers from a sleep disorder and is frequently ill. His parents are his sole caregivers. We feel invisible
- Institute for Patient- and Family-Centered Care. “Patient-and Family-Centered Care.” (2010), https://www.Ipfcc.org/about/pfcc.html
- Evidence Brief: Caregivers as Essential Care Partners. 2020. Evidence Brief: Caregivers as Essential Care Partners
- Hegelius et al. 2021. Consequences of visiting restrictions during the COVID‐19 pandemic: An integrative review. Consequences of visiting restrictions during the COVID‐19 pandemic: An integrative review - ScienceDirect
- Raphael et al. 2021. Unintended consequences of restrictive visitation policies during the COVID-19 pandemic: implications for hospitalized children. Unintended consequences of restrictive visitation policies during the COVID-19 pandemic: implications for hospitalized children | Pediatric Research (nature.com)